

Last week I started and ended my post incensed on behalf of my friend, who felt coldly and arrogantly dismissed by her new doctor. While I considered that his behavior may be influenced by his circumstances and did not attack his character or make generalizations based on gender, age, etc., I did blame him individually for how my friend felt in his presence.
Another friend read the post and said the doctor was not to blame, rather it’s the system. We exchanged thoughts and agreed that it was not all the doctor’s fault, and the whole healthcare system in our country is just a big mess in general. I continue to have daily conversations around physician well-being and systems transformation in medicine, and every single encounter advances my understanding of and awe at the whole situation. Here are my most current thoughts—bear with me, please.
3 Reciprocal Domains of Professional Fulfillment
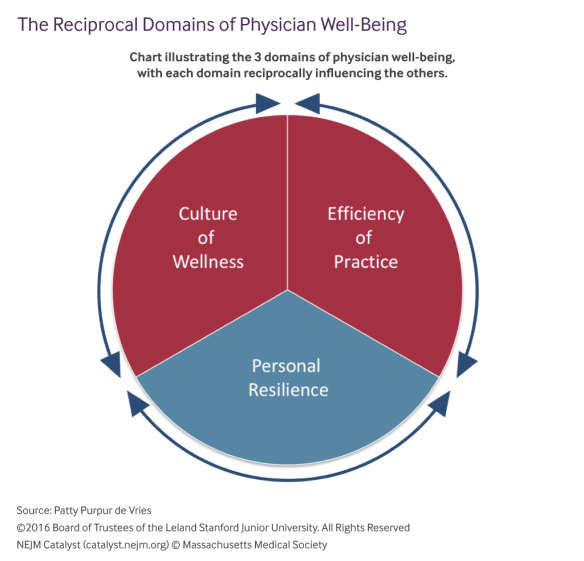
Most of us working in the physician well-being space have adopted a model for professional fulfillment developed by our colleagues at Stanford. If you care at all about your doctors’ professional health and how that impacts the care they deliver, I encourage you to read this article that describes their approach. In it, they define efficiency of practice (eg team workflow, electronic health record use and misuse, systems bureaucracy), culture of wellness (institutional attitudes that advocate for self-care, peer support, and mutual compassion between team members and patients), and personal resilience (individual skills and behaviors that promote personal well-being) as the three mutually influencing factors that determine, for individuals as well as organizations, our overall professional health and well-being:
The many drivers of both burnout and high professional fulfillment fall into three major domains: efficiency of practice, a culture of wellness, and personal resilience… Each domain reciprocally influences the others; thus, a balanced approach is necessary to build a stable platform that will drive sustained improvements in physician well-being and the performance of our health care systems.
For the record, I fully concur with this approach, and with one of the authors whom I met at the international conference in Toronto, that the most important parts of the framework are the arrows reminding us always to look for how the domains intersect and influence one another.
We Are the System
In the article, the authors write, “Efficiency of practice and a culture of wellness are primarily organizational responsibilities, whereas maintaining personal resilience is primarily the obligation of the individual physician.” This is where I differ somewhat. I fully agree that an organization’s culture is set at the top. Designated leaders lead by example, admit it or not, like it or not. They (and we—all doctors bear this responsibility on any given care team) provide cues for acceptable and unacceptable behavior, positive and negative.
That said, a team or an organization’s culture is executed and manifested day to day, moment to moment, in every interaction, by each individual within the system. This is the essence of complex systems—they are self-organizing at a global level (hence soon after joining a group we find ourselves adapting to fit in), and also emergent and evolutionary at the granular level (one person can turn a place around over time—have you seen it?). So in my opinion, both leaders and individuals are responsible for creating and maintaining the Culture of Wellness in medicine. We are the system. If you’re interested in more of what I think about this, check out this podcast from September 2018 when I presented to the surgeons and anesthesiologists at the University of Wisconsin at Madison.
In a Complex System, It’s All About Relationships
A person is a complex system. In my practice (and in my own life) I try always to attend to the relationships between 5 reciprocal domains (labelled intentionally after the Stanford model) of health: Sleep, Exercise, Nutrition, Stress Management, and Relationships. How do they relate? When I don’t get enough sleep I tend to overeat; when I eat too much I feel sluggish and unmotivated to exercise. When I exercise less I am more susceptible to stress, which puts my relationships at risk, which then disrupts my sleep, and the downward spiral persists.
A patient care team, a medical practice, a hospital—these are all complex systems. Besides the three domains in the Stanford model, what other factors contribute to the self-organizing nature of such systems? Perhaps individual autonomy, collective loyalty, shared mission, attention to training, and communication? What inter-relational factors dictate an individual’s or a subgroup’s behavior, and how does that influence the whole organization?
I am reminded of starlings in a murmuration, or sardines in a school. Seen from afar, the mass of animals appears to move as one agile and sentient organism. In reality, each animal’s movement is at once independent of and intimately tied to those in its immediate vicinity. Each animal’s awareness of and response to its neighbors are acute and instantaneous, respectively, and thus the collective is able to evade predators and give humans insight into what true multi-mutual cooperation looks like. They are attuned. This is possible because, according to science:
The change in the behavioral state of one animal affects and is affected by that of all other animals in the group, no matter how large the group is. Scale-free correlations provide each animal with an effective perception range much larger than the direct interindividual interaction range, thus enhancing global response to perturbations.
Would your organization, seen from afar, appear as organized and fluid as a flock of murmuring starlings? What would it require in order to do so?
* * * *
So what does this mean for my friend and how she (and we all) should think about doctors and our healthcare system in general? How does this actually relate to solutions to the problems I presented last week? Clearly, as I beat the long dead horse again and again, it’s about relationships, of course. But we have to think more deeply than just about our behaviors and actions—we’ gotta buckle up and dive into their origins—spelunk our default orientations toward self and others, our automatic settings, and how they manifest in our relationships and create, intentionally and not, our collective systems.
Once again, I have hit 1000 words on this post and it’s late. I’m getting there, I promise—not that I have the solution! I’m simply learning and synthesizing more every week about how we can more consciously and mindfully approach the problem. It has everything to do with the books I started reading recently about complexity, leadership, and mindset, and how they help me see my conversations and relationships in a new, exciting light.
More next week, friends!


