Suddenly I felt my heart pounding. My palms got sweaty. My jaw felt tense. I’m anxious, I realized. It felt like sometimes when I speak up in big meetings. Wow, I don’t even have to be in front of people for this to happen, how fascinating.
It was the second or third comment I had written on another Facebook page, belonging to a high school classmate. I think we became ‘friends’ through his wife, a friendly acquaintance of mine in high school, with whom I’ve been connected on Facebook for several years. I don’t really know her husband at all, and yet here I was, writing long replies on his page about universal masking, why recommendations changed between March and now, and why I trust Dr. Fauci despite his apparent flip-flop on this issue.
I had entered someone else’s house, offering my unsolicited opinions. Though we have a handful of mutual friends, I had no idea who else would attend this party, and whether I would be welcome. I wasn’t sure it was safe.
And yet I felt compelled to enter, why? Perhaps I felt defensive of my professional standard bearer, Dr. Fauci, the father of modern infectious disease and icon of science, medicine, and public health. He has basically led the research to define and defeat HIV/AIDS since the 1980s. Through six administrations, he has directed the National Institute of Allergy and Infectious Diseases (NIAID) to successfully manage H1N1, Ebola, and Zika, at home and abroad. He is one of my heroes. Likely, I also wanted to absolve myself a little, as I had also recommended against masking in public early on. I wanted to help some strangers see us, the ‘experts’, as human and fallible, and also earnest and caring, worthy of heeding.
So I obsessed over my comments. I read and reread before posting. I edited after posting. I included the links embedded above, inviting anyone on the thread to hear Dr. Fauci in his own words, in full. I offered my own mea culpa twice, explaining how academics sometimes fall victim to ivory tower thinking, as we did in this case. Perhaps this was my attempt at earning back whatever trust people may have lost because we experts contradicted ourselves in such an important and pivotal moment. I regret this, and I wanted people to know, and then maybe not hold it against me (us). Would I be crucified? Or would I crack a door open to hearing what I had to say? I feel anxious now, just thinking about it again.
My own friends discussed this on my page a few weeks ago, after my post on antibody testing (our recommendations have not changed yet). Paul, MD PhD and rheumatologist, pointed out, “US experts really blew it initially when it came to masks… All they had to do was consider the possibility that Asian countries might be right and then consider that the risk associated with (masking) was virtually zero. The first thing experts need to do, when confronted with circumstances that are truly new to them, is admit uncertainty and base recommendations accordingly.” I’m so lucky to have such honest and direct friends. I replied that I felt badly for following the ‘expert’ advice like a sheep (which is exactly how others on my acquaintance’s page described followers of universal masking, yikes). “Lesson learned,” I wrote—but have I really learned it? David, Paul’s and my classmate who now leads quality and hospitalist programs at his institution, replied, “It’s weird to be here with you (two) bashing experts, since the three of us are by any definition, experts. But the value of experts is not that they’re always right, but that they have a) a better track record and b) the ability to self-correct.” Yes, humility is key.
It all makes me wonder, how do we trust someone? I have conversations every day with patients and non-medical friends and family, educating and advising, and they are appreciative; they trust me. But we have already established mutually respectful, personal relationships. What made me think I could go on this unfamiliar man’s social media page, interact with perfect strangers, and have them trust or accept anything I said, when they had already expressed reservations about, if not hostility toward, my ‘tribe’? Was it my place?
The original post commented on universal masking and referenced Dr. Fauci not in a snarky, pejorative, or aggressive way. If it had I would have scrolled right by. Because it was a neutral presentation, I felt it could be safe to enter this house and offer my perspective. Out of respect for the page owner and his friends, I did my best to present both humbly and objectively, to be informative but not condescending. I really wanted to put my best online foot forward, to represent my tribe and my profession as well and as trustworthily (it’s a word!), as possible—to connect. So far I have not been attacked, and a few readers have liked my comments.
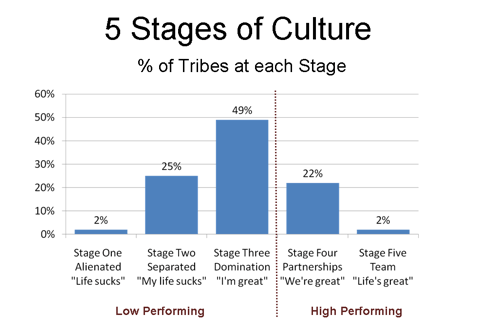
In the end, as I have written before, I think it’s about how we show up to one another. I wrote recently about tribal culture, and how through this crisis, individuals can help our own tribes thrive by modeling a more collaborative rather than competitive mindset, by amplifying our togetherness. “Who do we want to be on the other side of this crisis?” I asked. David Logan and colleagues go on in their work to discuss how tribes can effectively interact with other tribes, forming alliances and advancing even greater good together. They posit that tribes draw closer when their respective members, especially designated leaders (representatives), connect.
We find ourselves now in an existential battle for our lives, literally. Now is exactly the time to find common ground, step onto it, set up camp, and make decisions from there—to merge tribes. A friend asked me today, “Who do you want to be now?”
I want to be a connector, I answered. I will do my best not to contribute to division, polarization, alienation, disconnection, and suffering, through my words or actions. I will not be perfect. I will make mistakes. I will continue to learn and apply. I will strive to earn and maintain people’s trust. And I will help make it safe for people to question and challenge, discuss and explore any point of view. In the face of uncertainty, this is what I can offer.