NaBloPoMo 2018: What I’m Learning
Hi, I’m Cathy, and I’m addicted to my phone.
Last month I finally decided to do something about it, mostly so I could be more present to the kids. It’s been a fascinating journey so far, and I’m proud to say I’ve already made progress. First I banned Facebook after 6pm. That went well until I traveled. Then I took the Facebook app off of my phone. The withdrawl continues to spike at times. I also notice that I use other things to substitute—New York Times, email, Washington Post, email, WordPress Reader, email. I notice an anxiety, a frustration, a kind of crazed, darting hankering– I crave that dopamine hit.
The awareness of it all, however, and the commitment to get disentangled from my screen, has cleared space for a recently dormant impulse to surface afresh:
READ!
* * *
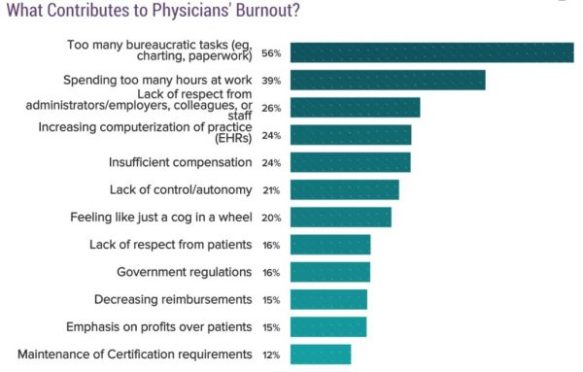
At the conference last month I was turned on to the idea of complexity (or chaos) theory and how it relates to fixing physician burnout and turning our whole medical system around. It was positively mind-blowing (for me—most others did not seem quite as lit). The speaker was Anthony Suchman, my newest hero. Some highlight ideas:
- Every system is perfectly designed to get exactly the results it gets. Our current healthcare system evolved to this point precisely from serial and cumulative decisions made over years, even though the current state was never the intent.
- We think of organizations as machines, with predictable, linear consequences of adjustments in one part or another. This is rarely how organizations (of people) actually work. Rather, we can think of organizations as conversations, and let go our expectations of particular outcomes, the illusion of total control. We can let things unfold and go where the outcomes lead us, all while holding to core values and goals.
- Patterns are (re)created in each moment, and also self-organizing. So at the same time that a pattern (eg culture) seems inevitable and self-propagating, sometimes small, almost imperceptible perturbations can create new and dramatic cascades that lead to transformation (the butterfly effect).
- Emergent Design thus embraces the approach of “finding answers we are willing to not know,” trusting that we will get where we need to go simply because we are paying attention (or that’s how I interpret it today).
This theory that everything within a system both results from and also contributes to the whole system (a fractal) validates an idea I have been advocating to my patients for years, and that I continue to personally relearn ad nauseam: It’s all connected. The most concrete examples are Sleep, Exercise, Nutrition, Stress Management, and Relationships—I used to call them the 5 Realms of Health; now I call them the 5 Reciprocal Domains. Each one is inextricably connected to every other one, and they all move in concert, with subtle or dramatic dynamics.

I browsed around my local bookstore a couple weeks ago and came across a colorful title on the shelf: Emergent Strategy by Adrienne Maree Brown. So of course I snatched it up. The blurb says:
Inspired by Octavia Butler’s explorations of our human relationship to change, Emergent Strategy is radical self-help, society-help, and planet-help designed to shape the futures we want to live. Change is constant. The world is in a continual state of flux. It is a stream of ever-mutating, emergent patterns. Rather than steel ourselves against such change, this book invites us to feel, map, assess, and learn from the swirling patterns around us in order to better understand and influence them as they happen. This is a resolutely materialist “spirituality” based equally on science and science fiction, a visionary incantation to transform that which ultimately transforms us.
Holy cow, YAAAAS!! I could not wait to read it! So I bought it, along with Make Trouble by Cecile Richards, What If This Were Enough? By Heather Havrilesky, and The Dharma of “The Princess Bride” by Ethan Nichtern. I had also ordered Leading Change in Healthcare, coauthored by Dr. Suchman and two others. That copy arrived last week.

I feel this as all part of a slow turn, getting off my phone and diving into books again. I’m so excited. I have done this before—buy a bunch of books and never read them. They occupy whole shelves in my bedroom. But I honestly feel a transformation coming on. Yesterday I spent a couple hours reading, researching, and writing the blog post, then I turned off the computer and opened Brown’s book. I read through the long introduction and resonated with sentences like, “Emergence is the way complex systems and patterns arise out of a multiplicity of relatively simple interactions.” This is a quote from Complex Adaptive Leadership: Embracing Paradox and Uncertainty by Nick Obolensky (which I have also now ordered). I also love (ha!), “Perhaps humans’ core function is love. Love leads us to observe in a much deeper way than any other emotion.” Also:
all that you touch
you change
all that you change
changes you
the only lasting truth
is change
god is change
That is a quote from Parable of the Sower by Octavia Butler.
Then before bed I opened Suchman et al’s book and found these words, also in the introduction:
Complexity theory here is enriched by the focus on relationships [Hallelujah!], rather than the more traditional reference to science. “Relationship-Centered Care” is a way of thinking that brings love and all that is personal into a world, the world of healthcare, that is mostly interested in more control and more data-based, evidence-based practices.
The point is made throughout that administrators cannot bring real change into their healthcare institutions without going through change themselves.
(The book describes) the relationship-centered social dynamics that are at the heart of Lean and a major source of this method’s success. Unfortunately, these social dynamics are overshadowed or even displaced by the analytic technique in some Lean implementations, compromising results.

So I’m learning about new ways to think on change. It’s changing how I approach trying to change my patterns, how I see my relationship to them, how I see all relationships. Wow.
All of this to say, I feel a deeply personal, yet global and cosmic impulse for growth, for transformation—a shift into more mindful and intentional use of my time and energy, and how I manifest it outward. Less distraction, more focus. Less incidental information consumption, more integrated learning and coordinated application. Less phone, more BOOKS.
What will be the outcome? I have no idea, that’s what makes it so exciting and wonderful! Onward!