

NaBloPoMo 2016, Letters to Patients, Day 27
To Patients Considering Full Body CT Scans:
Please reconsider.
Forgive me for putting on my preachy doctor hat for this post. I will also break my NaBloPoMo 500 word limit for this one.
As we approach the end of the calendar year, many of you may have met your health insurance deductibles. Maybe now would be a good time to get in some tests to ‘check under the hood,’ as some of you have said. I share below some of my screening recommendations, along with rationale.
Keep in mind that for this article, I define ‘screening’ as looking for a disease in a person with a) average risk for developing the disease and b) no symptoms.
Please also know that the opinions I express here are my own only and do not necessarily represent those of my colleagues, employer, or professional societies.
- Full body CT scan: This is not recommended by any clinical guideline or medical professional society as a screening test for anything. As I will describe below, specific screening tests are recommended for specific diseases, and the best ones obtain actual cells or tissue, rather than imaging alone. In addition, a full body CT exposes you to significant radiation, the long term consequences of which are still not fully understood. Lastly, CT scans inevitably detect incidental abnormalities that have no clinical consequences, but that often lead to invasive tests that can cause real harm, such as bleeding, pain, infection, and anxiety. This article from the FDA and this one by a radiologist at Harvard explain pretty clearly how the risks of this test far outweigh the benefits.
- Colonoscopy (colon cancer): This is the one test that nobody argues. It is both diagnostic (can see signs of early disease) and therapeutic (can take it out). Start at age 50, and repeat every 10 years if normal, barring new symptoms. Read the full guideline from the US Preventive Services Task Force (USPSTF) here. I know the prep is a pain, and I know you have to take a day off of work to have it. But on the whole, the returns here are well worth the investment.
- PSA and digital rectal exam (prostate cancer): This is perhaps the most personal decision of all cancer screening. Population-wise, we have yet to show mortality benefit from screening of any kind, such that the USPSTF now recommends against screening until better tests become available. But it’s not really that simple, because prostate cancer affects so many men, and is the second leading cause of cancer deaths in men in the US. The most important thing here is to decide which risks you are more comfortable with: potential serious harm from screening and unnecessary treatment, or finding cancer at a later, potentially more high-risk stage. This article from the New York Times may help, and this one from the National Cancer Institute.

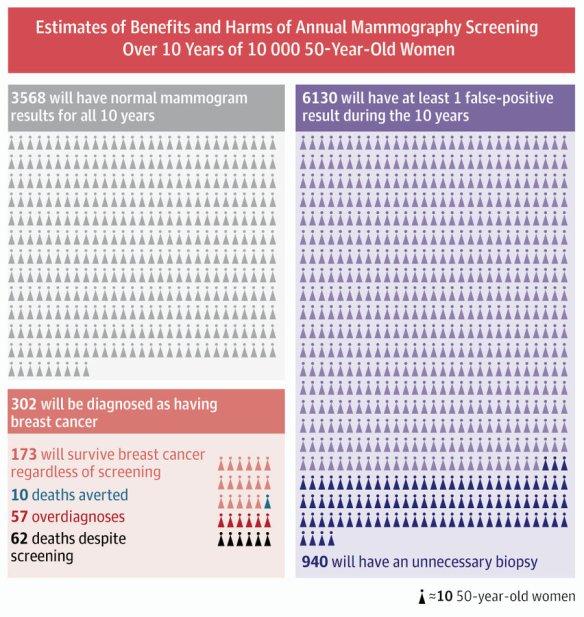
- Mammogram (breast cancer): It’s hard to walk back from more screening to less; people fear loss of security. When I started my training over 20 years ago, the recommendation was to screen every woman every year, starting at age 40. Since then epidemiologists have kept track, and similar to prostate cancer screening, the mortality rate from breast cancer has not decreased proportionally to the amount of screening done. Diagnosis has increased dramatically, due to early detection. Again, screening increases the risk of certain harms: anxiety (so much, for so many), pain, deformity, infection (from invasive biopsies), and then commitment to repeated testing (a vicious potential cycle of imaging, needling, more imaging, and more needling), while likely not saving your life. Here is the USPSTF guideline, and a helpful infographic . Like prostate cancer screening, this is one you have to decide for yourself, with the help of your doctor.
- Pap smear (cervical cancer): Again, former guidelines called for annual screening. Today, if your test is repeatedly normal and your sex habits are low risk, the interval can be lengthened to 3 to 5 years, and can start later in life (over 21). Cervical cancer is highly correlated to exposure to human papilloma virus, or HPV, which is sexually transmitted. Positive pap results, which range from mild to severe, occur far more often in younger women, and of those, many will revert to normal without progression to cancer in a woman’s lifetime. The main risk of over-screening, again, is unnecessary procedures when true disease not present.
In summary, these are the most common conversations I have with patients about screening. You may rightly infer that my personal bias is minimalist: Primum non nocere. Unfortunately, we have no good screening tests for some diseases, such as pancreatic cancer, ovarian cancer, and liver cancer, and the screening guidelines in other countries (eg Taiwan screens adults regularly for liver cancer) do not apply here because prevalence rates differ so widely.
This is why I think it’s important to establish care with a primary care physician and get regular check-ups. That fatigue you feel is likely just life and chronic sleep deprivation. You’re probably constipated because you eat too few stems/stalks/leaves and don’t move enough. You and your doctor can review your general health together, and if there is suspicion for some underlying health risk, it can be addressed personally and specifically.
To look up USPSTF guidelines yourself, I recommend searching Google for “USPSTF (disease) guidelines” and look for the hit that starts with “Final Recommendation Statement…” I have no financial or professional interests in Google or the USPSTF. Other respected sources for screening recommendations include the National Cancer Institute, the American Cancer Society, and the American Medical Association. As an internist, I recommend the American College of Physicians.
I hope this piece has helped illuminate the complex decision-making behind screening and diagnostic testing. I have only scratched the surface; the links contain the data and full rationale. Please take the time to read through them and discuss them with your doctor.


